.svg)

Reprogrammed Vascular Endothelial Cells (R-VECs) Are
Critical
“Missing Piece” for Therapeutic Organoids
Cell replacement therapies have demonstrated broad therapeutic potential, but long-term viability and teratogenic/neoplastic potential remain significant challenges. Whether allogeneic or autologously derived, transplanted cells lack the natural vascularization needed for full physiological integration
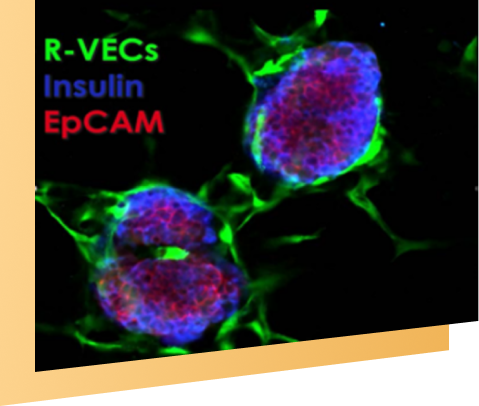
R-VECs are endothelial cells that naturally and permanently engraft into existing and generate entirely new vasculature through durable physiological processes